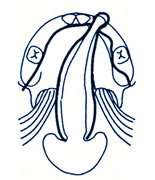
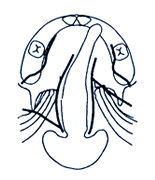
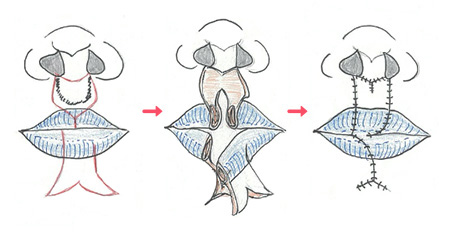
It was mentioned in detail earlier that cleft palate causes various problems. Palatoplasty is performed to solve these problems, but the purpose of this operation is not only to close the cleft but also to suture the splitted
soft palate muscle (levator veli palatini muscle), return it to a normal position, and reduce the dilated rhinopharynx.
If cleft palate surgery is performed too early, it will impair the growth of the upper jaw. However, if the surgery is delayed too much, the habit of abnormal pronunciation (abnormal articulation) will develop. Therefore,
in our department, surgery is performed at the age of around one year, when both of these conditions are satisfied fully, that is, before the baby starts active pronunciation exercise, and at the time when there is
as little growth of the upper jaw as possible. However, in reality, the timing may change a little depending on the condition of the baby at that time.
Moreover, there are cases where the palate surgery is completed in one stage and cases where the surgery is performed in two stages. The reason for dividing the surgery into two stages is to improve the growth of the upper
jaw as much as possible, but the optimal method changes depending on the condition of the mouth, so preoperative examination is performed to determine which method is better. Even in the case of the two-stage method,
the first palatoplasty is performed around the age of 1 year, and the second surgical hard palate closure is performed around the age of 1 year and 6 months to 2 years. The surgery is performed under general anesthesia,
and the length of the hospital stay is about 2 weeks.
Regarding the surgical method, we select the optimal surgical method for each patient from the following two surgical methods based on the width of the cleft, the length of the soft palate, and the state of muscle development.
In both surgical procedures, the surgery causes partial bone exposure of the upper jaw, so the entire upper jaw is covered with a celluloid cover until a new mucous membrane is formed to protect the wound. The period of
wearing it is about one week. Please eat soft meals for a while after discharge. After about 4 weeks after surgery, it is possible to return to the same diet as before surgery.
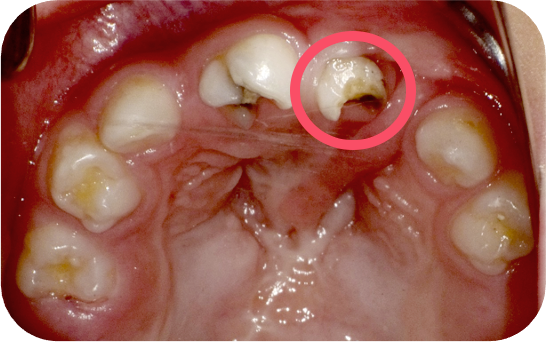
Additionally, since infants at this time put anything in their mouths, please be careful not to put any sharp objects (ball pens, chopsticks, etc.) into the mouth (please be especially careful until around 3 months after
surgery).
Regarding speech training, you will visit our division of Oral-Facial Disorders during the hospitalization to receive detailed explanations about future treatment (details will be described later).